
In the heart of Kenya’s capital, a once-revered institution teeters on the brink of oblivion. Nairobi Hospital, long hailed as the pinnacle of private healthcare for the nation’s elite and aspiring middle class, is unraveling under a mountain of debt, boardroom infighting, and brazen mismanagement.
A liquidation petition filed by security supplier Opticom K. Limited in August 2025 has laid bare the hospital’s financial rot, with debts soaring past Sh3 billion, unpaid bills to suppliers stacking up, and a deficit exceeding Sh1.2 billion in the last fiscal year alone.
Critics point to opaque loans, disputed procurements, and a leadership accused of incompetence CEO Felix Osano has become the face of this fiasco, with accusations of fiscal recklessness flying thick and fast.
But this isn’t just a tale of one hospital’s downfall; it’s a harbinger of systemic decay that mirrors the long-ignored collapse of Kenya’s public healthcare system. For years, the insulated middle class those with corporate jobs, SUVs, and private insurance has turned a blind eye to the rot in public facilities, believing their gated communities and premium plans shield them from the masses’ plight. How delusional.
The same forces eroding public health corruption, underfunding, strikes, and unequal resource distribution are now devouring the private sector’s crown jewel. And when Nairobi Hospital finally crumbles, as analysts warn it might, the ripple effects will slam into the middle class like a freight train, exposing their complacency as the suicidal arrogance it truly is.
Let’s not mince words: Kenya’s public healthcare is already a corpse, animated only by the desperate efforts of overworked, underpaid staff. Frequent strikes by health workers have paralyzed hospitals for months on end, leaving millions without care remember the 2017 debacle that ground the system to a halt for three months? Budget cuts have slashed funding by two-thirds in recent years, plunging counties into chaos with shortages of essential drugs like ARVs and TB treatments.
The rollout of the Social Health Insurance Fund (SHIF) in 2024 was a farce, with thousands unable to access treatment due to systemic failures and bureaucratic ineptitude. Unequal distribution means rural Kenyans die from preventable diseases while urban elites quibble over wait times.
A 2023 study highlighted weak budget monitoring and accountability as key culprits, allowing corruption to siphon funds meant for life-saving equipment. And in 2025, the crisis deepened: hospitals face severe shortages since January, with HIV patients scrambling for meds and women deprived of maternal care.
Now, witness the irony as Nairobi Hospital’s self-inflicted wounds echo these public sector horrors. In July 2025, the hospital jacked up charges by a staggering 61%, prompting eight major insurers to suspend services and leaving patients to foot exorbitant bills or seek alternatives. By August, that number swelled to 12 insurers pulling out, forcing the hospital to backpedal on the hike amid public outcry.
This isn’t innovation; it’s desperation. Boardroom wars have bled the institution dry, with factions decrying a “bleeding hospital” mired in deficits and questionable deals. The leadership malaise here is a microcosm of Kenya’s broader governance failures nepotism, opacity, and greed trumping competence.
The Rotten Core: Collusion Between Hospitals, Insurers, and the Ministry of Health
Peel back the layers, and you’ll find the true poison: a web of collusion between private hospitals, healthcare providers, insurers, and the Ministry of Health (MoH), all feasting on public funds while Kenyans bleed out. This isn’t mere inefficiency; it’s organized looting, where phantom hospitals ghost facilities that exist only on paper receive billions in remittances for services never rendered.
The National Hospital Insurance Fund (NHIF), now rebranded as the Social Health Authority (SHA), has been ground zero for these scams, with fraudsters siphoning off funds through fake claims, inflated bills, and non-existent clinics.
Enter Jayesh Saini, the shadowy tycoon whose empire spanning Bliss Healthcare, Lifecare Hospitals, Nairobi West Hospital, and entities like Minet and Medical Administrators Kenya Limited (MAKL) exemplifies this rot. Saini, often portrayed in puff pieces as a healthcare visionary, has been linked to siphoning Sh161 billion from the teachers’ medical cover deal over a decade, forcing educators into out-of-pocket payments at his facilities while pocketing premiums.

BOARDROOM THUG: Jayesh Saini linked to the collapse of Kenya’s healthcare system
Whistleblowers accuse him of masterminding fraud through Clinix Healthcare, where NHIF probes revealed payments to phantom entities. In 2025, Saini’s fingerprints are all over the National Equipment Support Program (NESP), a secretive leasing scheme brokered with the government, deducting up to 69% of SHA claims for equipment vendors and consortia, leaving public hospitals starved and dysfunctional.
This isn’t entrepreneurship; it’s predation, colluding with MoH officials and President Ruto’s inner circle to turn healthcare into a profit machine that kills Kenyans for gain.
And the Ministry? Complicit at every turn, from engineering NHIF’s swift closure into SHA to enable fresh scams, to ignoring antigraft probes that could recover billions. Recent exposés reveal how these networks exploit teachers and police officers, funneling funds offshore amid frozen accounts linked to money laundering trails.
Saini’s schemes don’t operate in isolation; they are bolstered by powerful allies like Adil Arshed Khawaja, the chairman of Safaricom and managing partner at Dentons Hamilton Harrison & Mathews (HHM).

HEALTHCARE THIEF: Adil Khawaja is behind Kenya’s healthcare woes, working under the direction of William Ruto
Khawaja, a close associate of President Ruto with over 30 years of legal maneuvering, has been instrumental in orchestrating the SHIF tender a KES 103 billion swindle that hands the digital backbone of Kenya’s healthcare to a consortium including Safaricom, Apeiro Limited (tied to Adani), and Konvergenz Network Solutions (linked to Nick Ruto).
Khawaja’s HHM firm pocketed hefty fees as transaction advisors, while Saini’s hospitals rake in payouts, ensuring a monopoly that starves public facilities.
This duo’s fingerprints are etched into the public healthcare collapse: SHIF, intended as UHC’s savior, has instead become a looting vehicle, with funds diverted to Saini’s empire and Khawaja’s enablers, exacerbating shortages, strikes, and deaths. Khawaja’s directorships in Saini’s outfits like NMC Fertility Kenya and Bliss Healthcare funnel public money into private pockets, while their political financing buys impunity.
Adding insult, Khawaja’s Safaricom has been accused of aiding state surveillance for abductions of critics, including those protesting healthcare failures, turning data into a weapon that silences dissent and perpetuates the rot.
But the rot festers even deeper through naked political patronage, as exemplified by Dr. Michael Bongei’s destructive tenure at Kenyatta University Teaching, Referral, and Research Hospital (KUTRRH). Appointed from State House and shielded by his cousin First Lady Rachel Ruto, along with former Principal Secretary Harry Kimtai, Bongei has turned this public beacon of affordable care into a personal fiefdom of fraud and favoritism.

Michael Bongei has been allowed to campaign while serving as a civil servant because he is related to Rachel Ruto
In mere months, he’s inflated procurement costs for essential supplies, extorting suppliers to fund his lavish home construction, while colluding with CEO Edward Maundu to dismantle the Hospital Management Information System (HMIS) erasing digital trails of theft. This sabotage, which forced the resignation of ICT Director Dr. Mwirigi Kiula for refusing complicity, mirrors the broader erasure of accountability in SHA and NHIF transitions.
Bongei’s tribalism stacks the deck with Kalenjin cronies, ballooning expenses and delaying care, while he brazenly campaigns for Bomet governorship in 2027 via “Bonga Na Bongei” initiatives all while drawing a civil servant salary, flouting the Public Service Code of Conduct and Leadership and Integrity Act.
The fallout? Skyrocketing costs at KUTRRH’s cancer center, postponed surgeries, endangered lives, and a staff restaurant on the verge of closure to pave way for outsourced profiteering.
This isn’t isolated incompetence; it’s the blueprint of patronage where Ruto family ties grant impunity, linking Bongei’s plunder to Saini’s and Khawaja’s networks in a symphony of greed that dooms public health.
Violations abound: from constitutional equality breaches in his abuse of female staff to anti-corruption laws shredded by his procurement scams, all unchecked by enablers like Rachel Ruto and Kimtai.
Exposés Shining a Light on the Vanishing Funds
Recent social media revelations have demanded answers over Ksh40 million vanished from SHA funds wired to Kandiege Sub-County Hospital in Homa Bay Ksh54.37 million disbursed, but only Ksh14 million reached patients.
This brazen theft at a public facility underscores how even county-level hospitals are ensnared in the fraud web, with funds disappearing into special purpose accounts without a trace.
These disclosures didn’t stop at Kandiege; they unveiled a damning list of SHA’s top payouts in June 2025, totaling billions funneled to 49 facilities many legitimate, but others reeking of insider deals and potential ghosts.
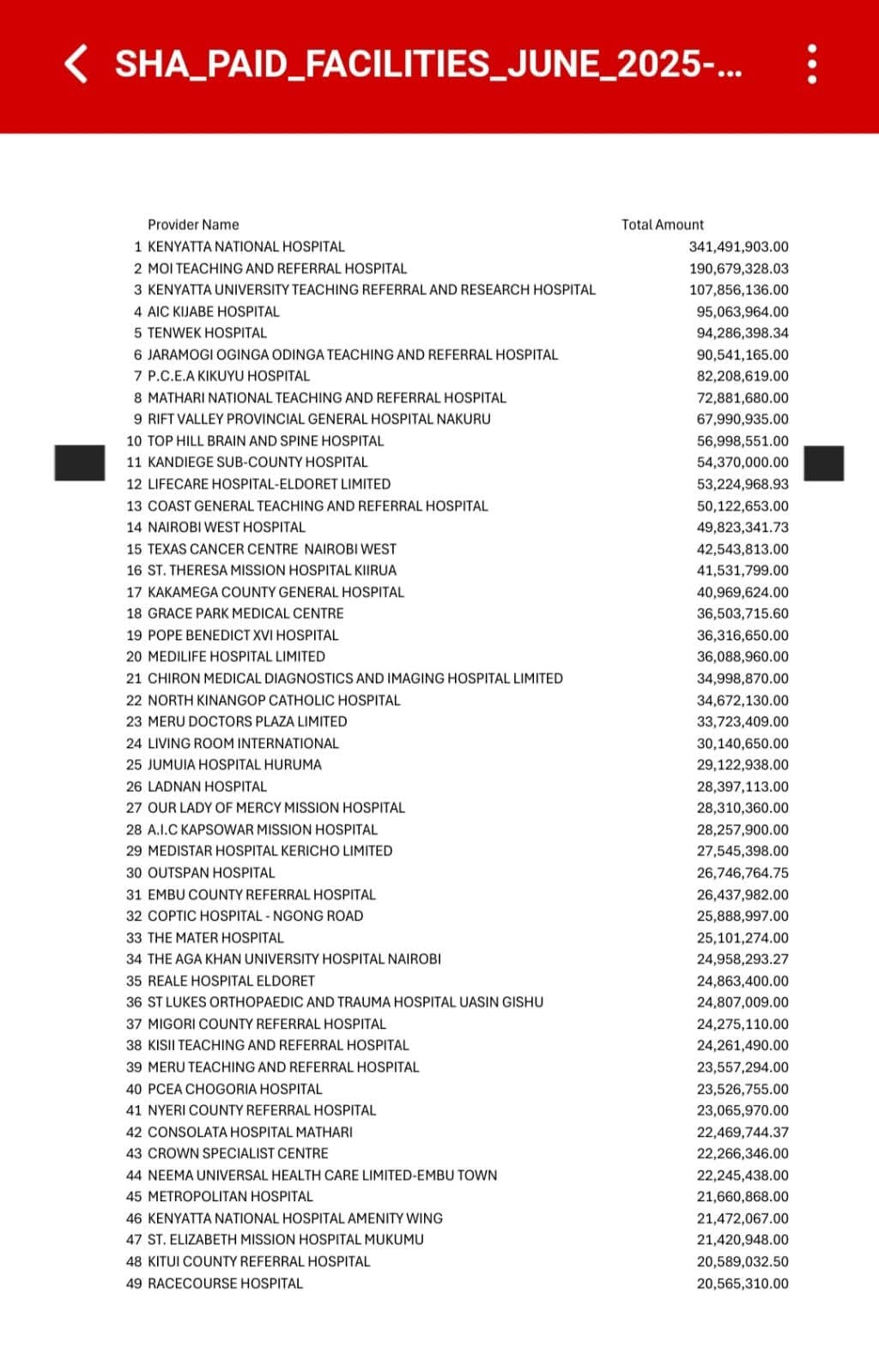
A list of hospitals which received SHA subventions but didn’t utilize it for actual healthcare interventions
Kenyatta National Hospital tops the chart with Sh341 million, followed by Moi Teaching and Referral at Sh190 million public giants sucking up funds while rural clinics starve.
But dig deeper: Lifecare Hospital-Eldoret Limited, part of Saini’s empire, pocketed Sh53.3 million, while Texas Cancer Centre Nairobi West another Saini-linked outfit under Nairobi West Hospital raked in Sh42.9 million. These aren’t coincidences; they’re the fruits of collusion, with Saini’s facilities built on a legacy of scandals from Clinix fraud to Sputnik V profiteering feasting on SHA remittances while patients suffer.
And it’s not just Saini. Ladnan Hospital, owned by SHA’s own chairman, snagged Sh28.3 million pure conflict of interest, as critics howl about fraudulent payments to insider-run entities. This list exposes the farce: billions vanish into a mix of public behemoths and private cronies, fueling strikes, shortages, and deaths.
Just days before these bombshells, the MoH suspended 40 facilities for fraudulent claims, a token gesture amid the looting. Yet, with Kandiege’s Sh40 million evaporated, how many more “special accounts” are black holes?
Oh, but the middle class thought they were immune. Sipping lattes in Westlands, they dismissed public health woes as the domain of the “unfortunate,” voting for (or ignoring) politicians who gutted budgets and devolved corruption to counties. They flocked to private havens like Nairobi Hospital, deluding themselves into believing their socioeconomic status elevated them above the fray a higher breed of human, untouchable by the chaos below. How aloof, how complacent.
Disease doesn’t check bank balances; cancer strikes the suited executive as readily as the street vendor. Economic analysts warn that the hospital’s potential liquidation will cascade through the economy, hiking costs and straining already fragile insurers.
When private options evaporate, where will this smug cohort turn? To the public system they’ve allowed to fester? Good luck. Strikes persist, with healthcare workers unpaid and demoralized, leading to 45-day disruptions in 2024 alone.
Performance assessments reveal vast disparities across counties, with poor accountability driving inefficiency. The middle class will bear the brunt: out-of-pocket expenses skyrocketing, families bankrupted by emergencies, and a rude awakening that their “premium” lives are built on sand.
This is no exaggeration it’s retribution for years of indifference. The collapse of Nairobi Hospital isn’t isolated; it’s the private sector catching the public disease, amplified by collusion and patronage that exposés lay bare.
If the middle class doesn’t wake up, demand accountability, and fight for systemic reform, they’ll soon join the queues they once pitied. Your daddy’s connections won’t save you now; the bill for complacency is due, and it’s payable in suffering.
